Functional Endoscopic Sinus Surgery (FESS) is one of the most widely performed minimally invasive procedures in otolaryngology. For clinicians, it represents the surgical standard of care for chronic rhinosinusitis (CRS) and related sinonasal conditions. For medical device manufacturers and OEM/ODM buyers, it represents one of the most consistently demanded application categories for rigid sinus endoscopes globally.
This article is written for both audiences. The first half covers the clinical foundations of FESS - what it is, who it is for, and how it works. The second half examines the instrument requirements and market context relevant to procurement teams and endoscope suppliers.
What Is Chronic Rhinosinusitis (CRS)?
To understand FESS, it is necessary to first understand the condition it primarily treats.
Chronic rhinosinusitis (CRS) is a symptomatic inflammatory disease of the nasal and paranasal mucosa lasting more than 12 weeks.¹ It is driven by complex interactions between structural and immune cells - including epithelial cells, lymphocytes, eosinophils, and neutrophils - producing inflammatory mediators such as cytokines, chemokines, and immunoglobulins.¹
CRS is far more prevalent than is commonly recognized. With a prevalence of approximately 11% in the general population, it significantly diminishes patient quality of life and productivity, and places a substantial burden on healthcare systems.¹ In the United States alone, CRS-related healthcare costs are estimated at $6.9–$9.9 billion per year.¹ The impact on patient quality of life is comparable to that of chronic diseases such as asthma, chronic obstructive pulmonary disease (COPD), and diabetes.¹
CRS Phenotypes
CRS is broadly classified into two main phenotypes, which are considered to have different aetiologies and pathomechanisms²:
- CRS with nasal polyps (CRSwNP) - characterized by benign inflammatory growths in the nasal and sinus mucosa, associated with type 2 inflammation and frequently co-occurring with asthma and aspirin sensitivity
- CRS without nasal polyps (CRSsNP) - the more common phenotype, typically associated with mucosal thickening and sinus obstruction without polypoid tissue
This distinction has direct implications for surgical planning, as the two phenotypes respond differently to medical and surgical treatment.
When Is FESS Indicated?
FESS is not the first line of treatment for CRS. Clinical guidelines recommend a stepwise approach beginning with medical management - including nasal corticosteroids, saline irrigation, and where appropriate, systemic antibiotics or biologics.
Surgery is considered when maximal conservative treatment has proven insufficient. Revision endoscopic sinus surgery (ESS) is often considered for CRS if maximal conservative treatment and baseline ESS both prove insufficient to control symptoms.³
Primary indications for FESS include:
- Chronic rhinosinusitis refractory to medical management
- Nasal polyposis causing significant obstruction or recurrence after medical treatment
- Acute complications of sinusitis (orbital or intracranial involvement)
- Mucoceles or sinus cysts
- Fungal sinusitis
- Benign sinonasal tumors requiring endoscopic resection
- Structural obstruction (e.g., concha bullosa, paradoxical middle turbinate) contributing to sinus drainage failure
The goal of FESS is not simply to remove diseased tissue, but to restore the natural drainage pathways of the paranasal sinuses - hence the term "functional." By reopening obstructed sinus ostia and removing disease while preserving as much normal mucosa as possible, FESS creates conditions for mucosal recovery and long-term symptom control.
How FESS Works: Surgical Overview
FESS is performed entirely through the nasal passages - no external incisions are required. The procedure relies on the rigid sinus endoscope to provide continuous, high-definition visualization of the operative field throughout.
A typical FESS procedure progresses through the following stages:
Pre-operative preparation The nasal cavity is decongested and anesthetized. In most centers, FESS is performed under general anesthesia, though local anesthesia with sedation is used in some settings. Preoperative CT imaging of the sinuses is essential for surgical planning and is reviewed alongside intraoperative endoscopic findings.
Initial visualization and uncinectomy The endoscope is introduced through the nasal passage. The first operative step is typically uncinectomy - removal of the uncinate process, a thin bony projection that partially covers the natural ostium of the maxillary sinus. This step opens access to the ostiomeatal complex, the critical drainage hub for the anterior sinuses.
Maxillary antrostomy The natural maxillary sinus ostium is identified and enlarged to improve drainage. A 30° or 70° endoscope is typically used here to visualize the lateral nasal wall and confirm ostial patency.
Anterior and posterior ethmoidectomy The ethmoid air cells - a labyrinthine network of small bony partitions between the nasal cavity and orbit - are systematically opened. This is the most technically demanding part of FESS, requiring precise endoscopic visualization to avoid injury to the orbit (lateral) and skull base (superior).
Frontal sinusotomy (if indicated) Access to the frontal sinus is achieved through the frontal recess. This is one of the most technically challenging aspects of FESS due to the narrow and variable anatomy of the frontal drainage pathway. A 70° endoscope is typically required for adequate visualization.
Sphenoid sinusotomy (if indicated) The sphenoid sinus is accessed via the natural sphenoid ostium. Given the proximity of the carotid artery and optic nerve, precise endoscopic visualization is critical.
Throughout all stages, the quality of the rigid sinus endoscope directly determines the surgeon's ability to identify anatomical landmarks, assess tissue character, and operate with precision. Image brightness, resolution, and geometric accuracy are not abstract specifications - they are functional prerequisites for safe surgery.
The Role of the Rigid Sinus Endoscope in FESS
The rigid sinus endoscope is the central instrument of FESS. Its optical performance governs the surgeon's situational awareness throughout the procedure, and its mechanical reliability determines whether that performance is maintained across the full duration of the case and across the full service life of the instrument.
Viewing Angle Selection
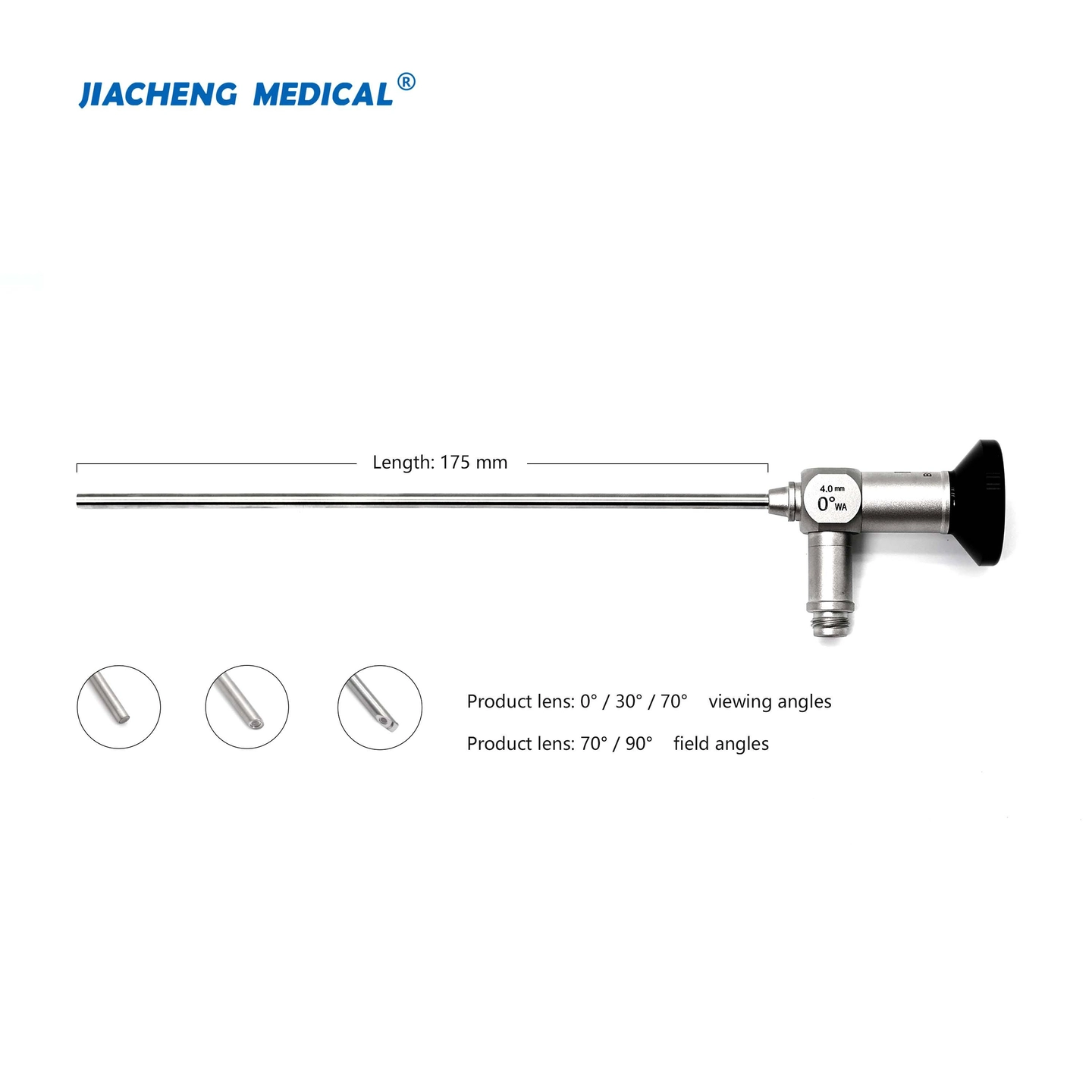
Different phases of FESS require different viewing angles:
|
Viewing Angle |
Primary Use in FESS |
|
0° |
Initial nasal cavity survey, septum assessment, sphenoid access |
|
30° |
Uncinectomy, maxillary antrostomy, ethmoidectomy - the workhorse angle for most FESS procedures |
|
70° |
Frontal sinus visualization, maxillary sinus inspection, hidden recesses |
The 30° endoscope is the highest-volume configuration in FESS and should form the core of any sinus endoscope product offering. The 70° scope is an essential complement for complete surgical coverage, particularly in frontal sinus procedures.

Optical Quality Requirements
The rod lens optical system - based on Harold Hopkins' design from the 1960s - remains the standard optical architecture for rigid sinus endoscopes. For FESS applications, the critical optical parameters are:
- Resolution sufficient to differentiate mucosal texture, identify anatomical landmarks, and detect early pathology at typical working distances of 5–30 mm
- Brightness adequate to illuminate the deep recesses of the ethmoid and frontal sinuses without requiring excessive light source intensity
- Color accuracy sufficient for tissue characterization - distinguishing healthy mucosa from inflamed, polypoid, or neoplastic tissue
- Low distortion to ensure accurate spatial perception, particularly near the skull base and orbit
Clinical Outcomes: What the Evidence Shows
FESS has a well-established evidence base demonstrating consistent clinical benefit in appropriately selected patients.
Symptom improvement rates following primary FESS for CRS are consistently reported above 80–85% in prospective studies and systematic reviews. The European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS 2020) - the most comprehensive clinical guideline in this field - provides detailed evidence grading for surgical indications and expected outcomes across CRS phenotypes.¹
However, not all patients achieve durable remission after a single procedure. Revision surgery is a recognized clinical reality, particularly in CRSwNP, where polyp recurrence rates are significant. Revision ESS is often considered when maximal conservative treatment and baseline ESS prove insufficient.³ Factors associated with revision surgery include CRSwNP phenotype, comorbid asthma, aspirin-exacerbated respiratory disease, and incomplete primary surgery.
This revision surgery dynamic has direct implications for instrument demand: patients requiring revision procedures represent a sustained source of surgical volume at ENT centers, supporting long-term demand for sinus endoscope consumables and replacement instruments - a dynamic that shapes both inventory strategy and product lifecycle planning for OEM/ODM suppliers.
The clinical dynamics described above - sustained surgical volumes, high revision rates, and growing adoption in emerging markets - translate directly into structural instrument demand. The following section examines what this means for procurement teams and OEM/ODM suppliers.
FESS Market Overview: Procurement and OEM Perspective
Global Procedure Volume and Growth Drivers
FESS is performed across all major healthcare markets. The global burden of CRS - with a prevalence of approximately 11% and annual US healthcare costs of $6.9–$9.9 billion¹ - sustains high and growing surgical volumes in North America, Europe, and increasingly in Asia-Pacific markets where ENT surgical infrastructure is expanding.
Key demand drivers include:
- Rising CRS prevalence, driven in part by urbanization, air quality, and allergic comorbidities
- Growing adoption of FESS as the surgical standard of care in emerging markets
- Increasing revision surgery rates as treated patient populations age and require retreatment
- Expansion of endoscopic techniques into adjacent ENT applications (skull base surgery, dacryocystorhinostomy, orbital decompression)
Instrument Demand Structure
A typical FESS setup requires a minimum set of rigid sinus endoscopes covering the three standard viewing angles (0°, 30°, 70°) in the standard adult diameter (4 mm). High-volume ENT centers maintain multiple sets to allow concurrent sterilization and continuous surgical throughput.
Pediatric ENT departments additionally require 2.7 mm diameter scopes for age-appropriate anatomy.
Instrument replacement is driven by:
- Optical degradation after extended sterilization cycles (typically 300–500+ cycles for well-manufactured instruments)
- Mechanical damage from intraoperative handling or transportation
- Upgrade cycles as centers transition to HD or 4K camera systems requiring compatible endoscope interfaces
For OEM/ODM buyers, understanding this replacement cycle dynamic is important for inventory planning and account management at hospital system level.
Compliance Requirements for Market Access
Sinus endoscopes supplied into FESS applications must meet the full suite of applicable international standards. The regulatory requirements vary by market:
|
Market |
Key Requirements |
|
European Union |
CE marking under EU MDR (2017/745) |
|
United States |
FDA 510(k) clearance, QSR compliance |
|
Global OEM baseline |
ISO 13485, ISO 8600 series, ISO 14971 |

For a detailed breakdown of each standard and its implications for OEM endoscope manufacturing, see our [Sinus Endoscope compliance guide →].
Conclusion
FESS represents both a mature clinical standard of care and a structurally robust market for rigid sinus endoscope suppliers. For clinicians, the procedure offers a well-evidenced, minimally invasive approach to CRS management with strong long-term outcomes in appropriately selected patients. For procurement teams and OEM/ODM partners, it represents a high-volume, compliance-critical application where instrument optical quality directly determines surgical outcomes - and where product reliability, compliance documentation, and supply consistency are the primary purchasing criteria.
contact us
Looking for rigid sinus endoscopes for FESS applications? [View our product specifications →] or [contact us →] for OEM/ODM customization, compliance documentation, and sample requests.
Related articles
[ Rigid Sinus Endoscope Guidelines→]
[ How to Source Medical Endoscopes from China→]
Related Products
[Sinoscope | 0° / 30° / 70° →]
[ Sinoscope - Value Series | 0° / 30° / 70°→]
[Professional Arthroscope | 0° / 30° / 70° →]
[ Rigid Laparoscope | 0° / 30°→]
References
- Fokkens W, Lund V, Hopkins C, Hellings P, Kern R, Reitsma S, et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology. 2020;58(Suppl S29):1–464. doi: 10.4193/Rhin20.600
- Fokkens WJ, Lund VJ, Mullol J, et al. European position paper on rhinosinusitis and nasal polyps 2012. Rhinol Suppl. 2012;23:3.
- Nuutinen M, Haukka J, Virkkula P, Torkki P, Toppila-Salmi S. Using machine learning for the personalised prediction of revision endoscopic sinus surgery. PLoS One. 2022 Apr 29;17(4):e0267146. doi: 10.1371/journal.pone.0267146. PMID: 35486626; PMCID: PMC9053825.